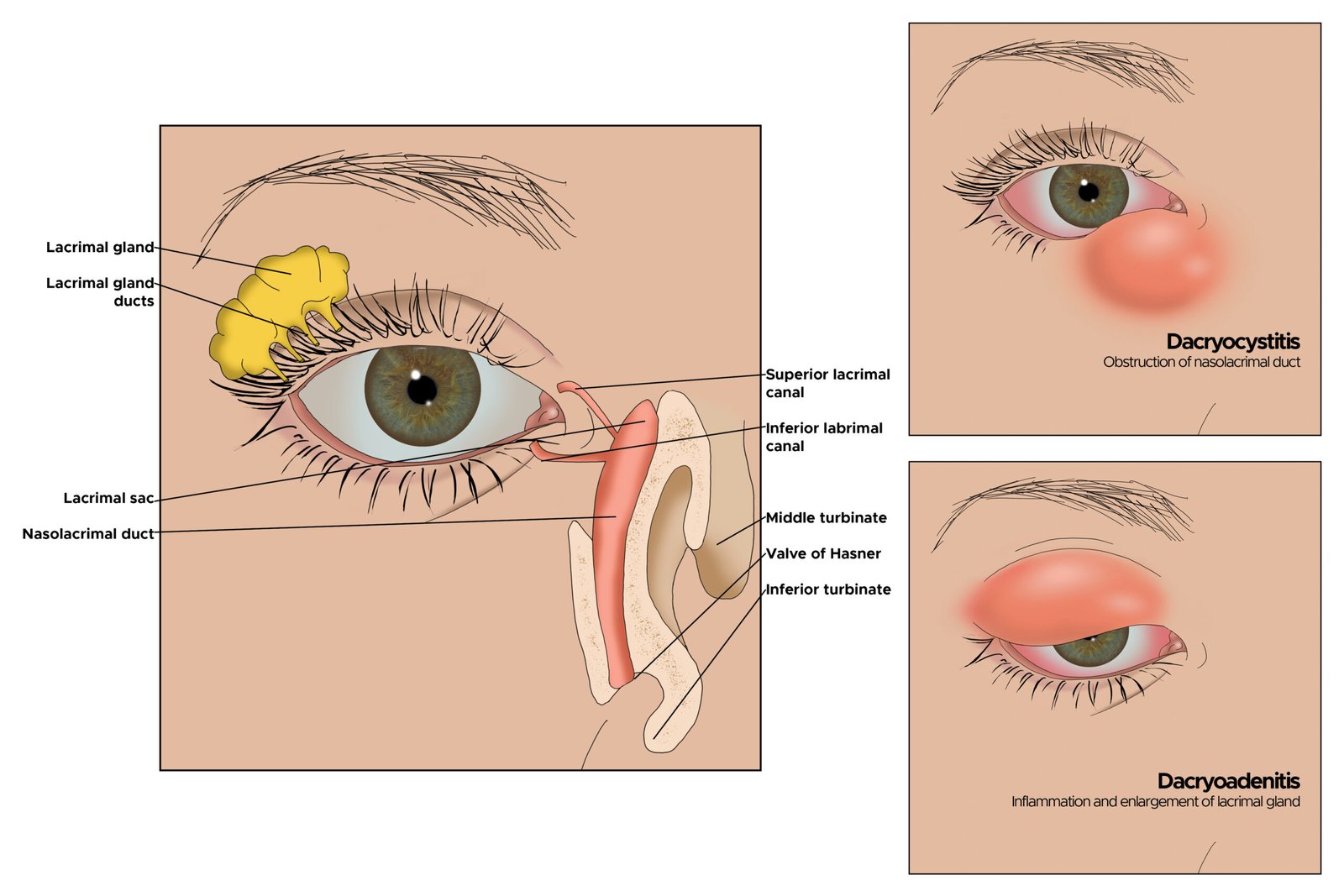
Dacryostenosis (also known as nasolacrimal duct obstruction or blocked tear duct) is a condition in which the tear drainage pathway (nasolacrimal duct) is narrowed or blocked, preventing tears from draining properly from the eye into the nose. It is very common in newborns (congenital form) and can also occur in adults (acquired form). In infants, it often resolves spontaneously within the first year of life, but persistent cases may lead to watery eyes or secondary infection. In homeopathy, remedies are used only as supportive care to help reduce excessive tearing, discharge, and inflammation while supporting natural drainage. Dacryostenosis requires evaluation by an ophthalmologist, especially if there are signs of infection.
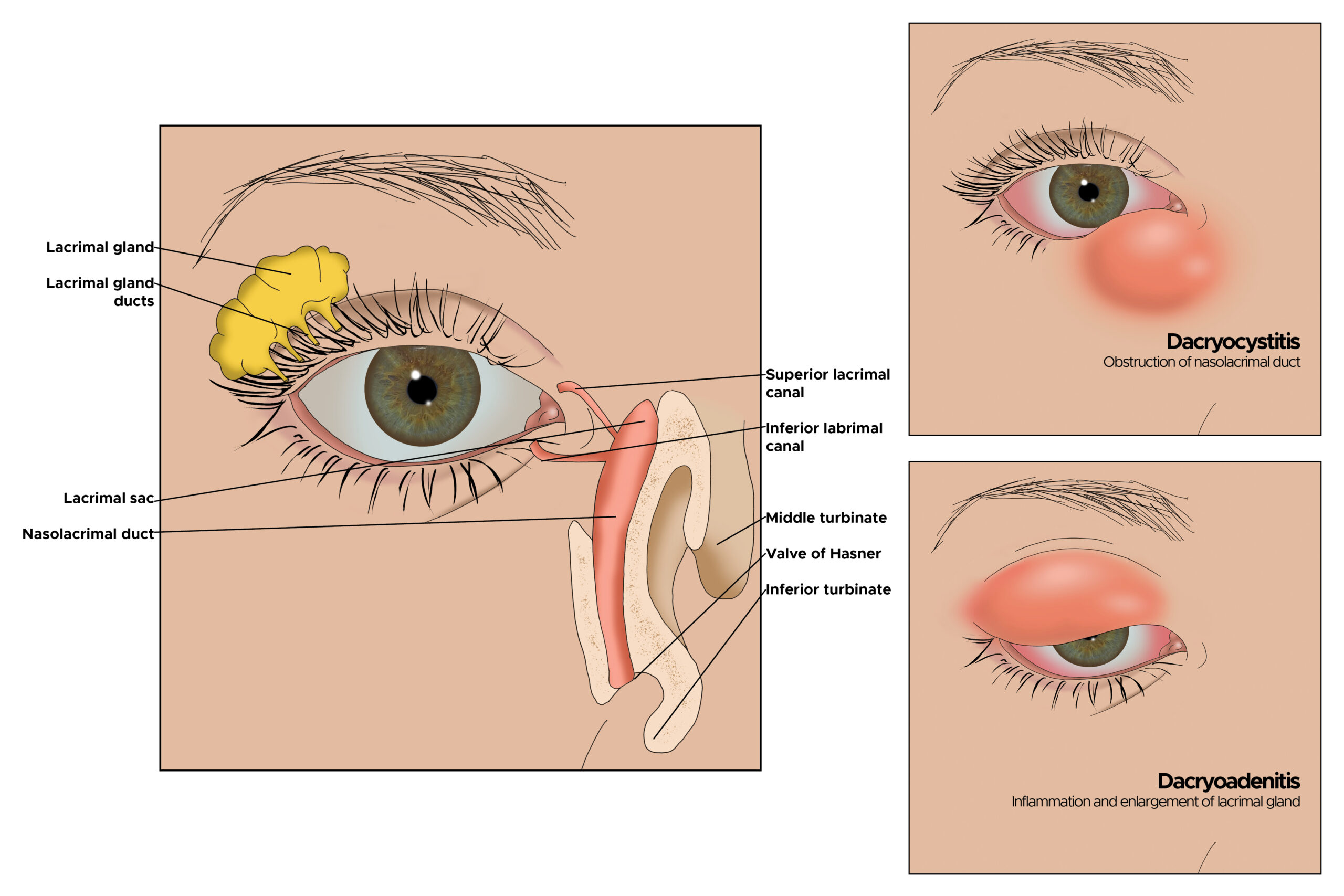
(Images above show dacryostenosis/blocked tear duct — excessive tearing, mucoid or purulent discharge at the inner corner of the eye, and possible swelling of the lacrimal sac.)
Causes
Dacryostenosis occurs due to:
- Congenital: Failure of the thin membrane (valve of Hasner) at the end of the nasolacrimal duct to open properly at birth
- Acquired: Inflammation, scarring, infection, trauma, tumors, or nasal polyps blocking the duct
- Poor drainage leading to stasis of tears and secondary bacterial overgrowth
Symptoms
Common symptoms include:
- Persistent watery eyes (epiphora) or overflow of tears even without crying
- Mucoid or sticky discharge at the inner corner of the eye, especially in the morning
- Crusting or matting of eyelashes
- Mild redness or swelling near the inner corner (lacrimal sac area)
- In infected cases (dacryocystitis): painful swelling, redness, pus, and fever
Homeopathy Medicines with Key Symptoms and Doses
Homeopathic remedies for dacryostenosis are selected based on the type of discharge, inflammation, and the person’s (especially infant’s) constitution. The following are commonly considered for supportive management. Remedy selection must be determined only by a qualified homeopath after detailed case-taking, in coordination with an ophthalmologist. These are general guidelines only. Gentle lacrimal sac massage (Crigler maneuver) as taught by a doctor is often the first-line approach in infants.
Pulsatilla For mild, changeable symptoms with thick, bland, yellowish-green discharge. The child is weepy and better in open air. Often useful in infants. Typical use: 30C, 3-5 pellets 1-2 times daily.
Mercurius Solubilis For offensive, purulent discharge with swelling and pain worse at night. Excessive salivation or bad breath may be present. Typical use: 30C, 3-5 pellets 1-2 times daily (short term).
Silicea For slow resolution with tendency to suppuration or recurrent discharge. Supports drainage and tissue strength. Typical use: 6X or 30C, 3-5 pellets 1-2 times daily.
Euphrasia Officinalis For profuse, acrid (burning) tearing with redness and sensitivity to light. The discharge may irritate the skin. Typical use: 30C, 3-5 pellets 1-2 times daily.
Natrum Muriaticum For clear, watery discharge with dry or raw feeling around the eyes, often linked to emotional factors. Typical use: 30C, 3-5 pellets 1-2 times daily.
Apis Mellifica For puffy swelling with stinging or burning pain and thirstlessness. Better from cold applications. Typical use: 30C, 3-5 pellets 1-2 times daily (short term).
Belladonna For sudden redness, throbbing pain, and heat with feverish symptoms. Typical use: 30C, 3-5 pellets 1-2 times daily (short term).
Hepar Sulphuris For very sensitive, pus-forming cases with stitching pain. Better from warmth. Typical use: 30C, 3-5 pellets 1-2 times daily (short term).
Calcarea Carbonica For fair, sweaty infants with constitutional sluggishness and recurrent discharge. Typical use: 30C or 200C, 3-5 pellets once or twice weekly.
Sulphur Often used as an intercurrent remedy in chronic or recurrent cases with unhealthy tendency or burning. Typical use: 30C or 200C, sparingly (once weekly under guidance).
Important guidance: Most congenital dacryostenosis in infants resolves spontaneously by 6–12 months with gentle massage of the lacrimal sac (Crigler maneuver) several times daily. Warm compresses and antibiotic drops/ointment are used if infection develops. Persistent cases after 12 months may need probing or surgery by an ophthalmologist. Homeopathy may help reduce tearing, discharge, and inflammation as supportive care but must never replace proper eye care and medical follow-up. Keep the eye area clean and avoid rubbing. This information is for educational purposes only and not a substitute for professional medical or homeopathic advice. Consult a qualified ophthalmologist (especially for infants or if there is swelling, pus, or fever) for accurate diagnosis and management, and a registered homeopath for individualized supportive remedy selection. With timely care, most cases resolve well without long-term issues.